
And Yet Another Tale of Two Maps
My recent series on diet and cardiovascular health has produced some interesting findings. Within these findings, I have noticed some intriguing patterns. Following in the tradition of my “Tales of Two Maps” series, here are another set of two maps:

This is the previously featured map of the year 2000 mortality rate from cardiovascular disease in Europe, drawn from here. As we see, there is a distinct northeast to southwest cline. (Although not highlighted here, rates are significantly higher in Russia; if it were colored, it would be very much bright red.)
I wanted to know if there was any simple explanation for this obvious geographic pattern, and then a look back at one of my previous posts gave me a clue:


This is a map of average minimum winter temperatures across Europe. Note how this map correlates to the above map almost perfectly. While the climate of Europe has varied considerably over the ages, we can still get a rough idea of how things were in the past.
But why does this matter? Well, Europeans have been farming for many thousands of years. In the colder climates, growing seasons were shorter. This meant that bulking up on calories was critical during the warm months, to help to survive the long, cold, dark, and very lean winters.
To get an idea of what this has done to modern European populations, see this passage in the previously cited Rob Dunn article:
A Body is Not a Body—Amazingly, there are more ways in which a calorie is not a calorie. Even if two people were to somehow eat the same sweet potato cooked the same way they would not get the same number of calories. Carmody and colleagues studied a single strain of heavily inbred lab mice such that their mice were as similar to each other as possible. Yet the mice still varied in terms of how much they grew or shrank on a given diet, thanks presumably to subtle differences in their behavior or bodies. Humans vary in nearly all traits, whether height, skin color, or our guts. Back when it was the craze to measure such variety European scientists discovered that Russian intestines are about five feet longer than those of, say, Italians. This means that those Russians eating the same amount of food as the Italians likely get more out of it. Just why the Russians had (or have) longer intestines is an open question. Surely other peoples differ in their intestines too; intestines need more study, though I am not going to volunteer to do the dirty work. We also vary in terms of how much of particular enzymes we produce; the descendents of peoples who consumed lots of starchy food tend to produce more amylase, the enzyme that breaks down starch. Then there is the enzyme our bodies use to digest the lactose in milk, lactase. Many (some say most) adults are lactose deficient; they do not produce lactase and so do not break down the lactose in milk. As a result, even if they drink milk they receive far fewer calories from doing so than do individuals who produce lactase. Each of us gets a different number of calories out of identical foods because of who we are and who our ancestors were.
(emphasis added)
Russians (on one end of the spectrum) have evolved to more thoroughly extract the calories from their food than Italians (who are on the other end of the spectrum). I wouldn’t be surprised if other Europeans fall in between in intestinal length, in accordance with the above maps.
In addition to varying on the amount of calories extracted from food, people vary in what their bodies do with those calories:
Ultimately, the relationship between physical activity and fatness comes down to the question of cause and effect. Is Lance Armstrong excessively lean because he burns off a few thousand calories a day cycling [Jayman: or injected a few thousand units of performance enhancing substances, but anyways], or is he driven to expend that energy because his body is constitutionally set against storing calories as fat? If his fat tissue is resistant to accumulating calories, his body has little choice but to burn them as quickly as possible: what Rony and his contemporaries called the “activity impulse”—a physiological drive, not a conscious one. His body is telling him to get on his bike and ride, not his mind. Those of us who run to fat would have the opposite problem. Our fat tissue wants to store calories, leaving our muscles with a relative dearth of energy to burn. It’s not willpower we lack, but fuel.
For the last 60 years, researchers studying obesity and weight regulation have insisted on treating the human body as a thermodynamic black box: Calories go in one side, they come out the other, and the difference (calories in minus calories out) ends up as either more or less fat. The fat tissue, in this thermodynamic model, has nothing to say in the matter. Thus the official recommendations to eat less and exercise more and assuredly you’ll get thinner. (Or at least not fatter.) And in the strict sense this is true—you can starve a human, or a rat, and he will indeed lose weight—but that misses the point. Humans, rats, and all living organisms are ruled by biology, not thermodynamics. When we deprive ourselves of food, we get hungry. When we push ourselves physically, we get tired.
[…]
From this biological or homeostatic perspective, lean people are not those who have the willpower to exercise more and eat less. They are people whose bodies are programmed to send the calories they consume to the muscles to be burned rather than to the fat tissue to be stored—the Lance Armstrongs of the world. The rest of us tend to go the other way, shunting off calories to fat tissue, where they accumulate to excess. This shunting of calories toward fat cells to be stored or toward the muscles to be burned is a phenomenon known as fuel partitioning.
(emphasis mine)
In short, evolution may have conditioned various people to respond differently to food based on their ancestors’ level of food availability (and effort required to get it). In the balmy Mediterranean parts of Europe, food was probably more available all year round, reducing the need for the inhabitants to develop super-efficient digestive systems. Today, when exposed to the rich supply of foodstuffs of all sorts today, their bodies are better able to tolerate it.
By contrast, those in the colder, snowier Northern and Eastern parts of Europe may have evolved a stronger desire to consume food whenever it’s available, particularly carbohydrates. (However, northern Europeans don’t seem to be more prone to storing fat, as this map indicates, with the exception of the Brits–as with their American offshoots.) Northern and Eastern Europeans may faced a trade-off with their efficiency at absorbing and processing calories coming at the cost of long-term cardiovascular health.
Interestingly, the map of winter temperatures, particularly the 0° C isotherm seems to correlate well to the points in Spain and Italy where average IQ starts to drop, as I’ve noted previously.
The drop in hearth health in Britain may have something to do with the lower levels of sunlight it receives, which may stunt farming there. As well, the drop in heart health (and IQ) that occurs in the Celtic fringes may be do to the history of pastoralism there, thanks to the rockier and poorer quality soil (very evident in Scotland).
Greece may be an outlier in cardiovascular health thanks to its very high rate of smoking [Edit: also see here].







Also, with far lower number of annual hours of bright sunshine further north ( for Britain, see: http://metofficenews.wordpress.com/2011/06/23/met-office-in-the-media-23-june-2011/ ), inevitably there are higher rates of Vitamin D deficiency at these latitudes. Vitamin D deficiency increases risk of heart disease, according to a Danish study ( see: http://www.sciencedaily.com/releases/2012/09/120924102504.htm ). And as it happens, Scotland has far higher rates of early deaths from heart attacks versus southern England (although this is compounded by lifestyle factors also).
While that’s certainly interesting, the study appears correlational. Hence, it’s not clear if that relationship is causal.
I’m still seeing the rust of the Iron Curtain, somewhat more than temperature. Otherwise, why are the Bavarians and Swiss healthier than Croats?
Croats are Slavs 🙂 So they may come from the stock, which (because of original environment) is somewhat more susceptible to the factors causing heart diseases.
The deaths from cardiovascular disease map also correlates with the World Health Organization’s alcohol-attributable deaths as a percentage of total deaths map (2004):
It has been suggested that under communism, rates of alcoholism greatly increased in eastern European countries. In addition, alcoholism is known to contribute to vitamin and mineral deficiencies. Since certain vitamins and minerals play a key role in heart health, a deficiency in these vitamins and minerals caused by alcoholism, combined with general poor nutrition, stress, high rates of smoking, and lack of sunlight at some of the higher latitude countries, in my opinion accounts for higher rates of death from cardiovascular disease in the eastern European countries on the original map.
Independent of your main point is that would be another example of a tale of two maps – a sorely untapped source of low-hanging fruit imo.
Thanks. That was my thought too.
Quite possible. But is that THE thing? That’s the question.
Taken from:-
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1121549/
Understanding the toll of premature death among men in eastern Europe
Martin McKee, professor of European public health and Vladimir Shkolnikov, head of the laboratory of demographic data
Cardiovascular disease
“Mortality due to cardiovascular disease is greatest, relative to western Europe, in the age group 35-44. Cardiovascular disease is understood differently in Russia, in several important aspects, than in western Europe. Thus, mortality for cardiovascular disease is especially high at young ages. Deaths are also more likely to be sudden,14 and many people who die show little evidence of the expected coronary artery lesions.15 The traditional risk factors identified in western epidemiological research, such as smoking, lipid levels, and physical activity, have little predictive value.16 Indeed, lipid metabolism appears to differ in Russians and Americans.17 Instead there is growing evidence that other factors are involved. Eastern European diets, for example, are characterised not only by large amounts of fat but also by very low quantities of fruit and vegetables. Correspondingly, antioxidant activity in the blood is extremely low.18,19 The role of micronutrients in macrophage adhesion and passage of cholesterol through arterial walls provides a mechanism by which this could cause heart disease.20 The rapid reduction in cardiovascular deaths in some countries, coinciding with changes in diet, offers support for this hypothesis.21,22 Poor nutrition is thus likely to be important in explaining the overall difference in mortality compared with western Europe. Although there are some differences in the diets of men and women,23 the differential impact on health is likely to be small.
Another factor that contributes to increased mortality due to cardiac disease is alcohol. Across northern Europe, but especially in Russia and some of its neighbours, alcohol is typically drunk as vodka and in binges,24 in contrast to a more steady consumption in southern and western Europe. A possible link with cardiac death was suspected following the observation that deaths in Moscow from cardiovascular disease increased at weekends, a finding incompatible with the effects of the traditional risk factors.25 (This was later replicated in Scotland,26 indicating the wider implications of research in eastern Europe). Binge drinking is associated with a marked increase in the risk of cardiovascular death, and in particular sudden cardiac death,27 reflecting different physiological responses to binge drinking and regular moderate consumption.28 A third factor, although one whose role is less well defined, is the high level of psychosocial stress.29..”
I also think peoples whose diet was dominated by pastoralism the longest (because crops didn’t grow well in their latitude or climate until relatively recent times compared with meditteranean latitudes) will have a different tolerance to alcohol.
Quite possibly. Perhaps that explains the Celts, who are known for their drinking…
Interesting. Maybe that’s the kicker…
Hello Jayman,
you may have covered this and I’ve not spotted it – fat cells have a feedback loop – presumably to deal with areas prone to drought – after a period of very low food intake, fat cells increase their ability to retain fat globules – hence crash dieting is the worst strategy possible. That feedback loop is presumably not uniform amongst people either, and may depend on haplogroup/other migration ancestry of a person.
A thought about gut length (prob something else you already know) my understanding since way back when, has been that gut length relates to the ease/difficulty of breaking down the food. Cellulose requires more stomach and gut. Wheat and rye may be harder to digest than rice. Rye has the additional problem of alkaloids and may need extra time to deal with the toxins. [I came across this interesting page whilst checking the spelling of alkaloids http://waynesword.palomar.edu/ww0703.htm%5D
bw BNK
Thanks! I think intestinal length is probably only part of the story. More importantly, it speaks to overall metabolic differences across different European groups that might contribute to what we see here. It is possible that these different groups would do differently if they had diets more suited to them, as we see suggested above.
Apparently cold temperatures cause vasoconstriction which may partly explain higher rates of heart attacks during winter months. During cold temperatures bloodflow shifts from the peripheries of the body to the centre, and the body reacts by getting rid of some fluid to make room for the increased blood volume. These fluid shifts increase the likelihood of clotting, which likely partially accounts for the increased cardiac problems during winter or in countries with colder climates. Needless to say, smoking also causes vasoconstriction and contributes to heart disease, and many eastern European countries have high smoking rates: http://en.wikipedia.org/wiki/List_of_countries_by_cigarette_consumption_per_capita
“Apparently cold temperatures cause vasoconstriction which may partly explain higher rates of heart attacks during winter months.”
Doesn’t alcohol exacerbate that? I vaguely recall first aid lectures where it was said giving alcohol to people with hypothermia was a bad idea?
Thanks! Great find, I will incorporate this into the main post.
US heart attack rates/ethnicity/seed zone
http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_men_heart.htm
http://www.forestseedlingnetwork.com/resources/seed-zone-maps/other-maps/usda-hardiness-zones.aspx
Thanks. The thing that limits the useful this however is that self-reported ancestry is a bit unreliable. There does seem to be a pronounced elevation of cardiovascular mortality in the Scotch-Irish areas however, consistent with the elevated rates among the Celts in Europe.
Applause. If this is your original finding, very very good.
These graphics would look great on the cover of Science magazine or Nature, if they are interested in either science or nature.
Thanks! Well, it is my own discovery, but I don’t know if I’m the first one to spot it.
In f.USSR alcohol overwhelms all other factors as contributors to heart attacks. For instance, Russia’s life expectancy went from 67.7 years in 1984 to 70.0 in 1986-7, that is, in a mere two years, in the period coinciding with Gorbachev’s much-maligned alcohol campaign. In general, Russian life expectancy in modern times, including mortality from cardio-vascular diseases (which accounts for c.60% of all deaths), has closely tracked alcohol consumption. Here is a graph which plots mortality (black) vs estimated alcohol consumption (green) until 2003.
Interesting. Perhaps this is so.
your explanaition might be interesting it doesn’t manage to explain the strong and sharp difference taht exist between the regions of the northern border of France and their neiboring German or English regions. There is not a sharp climate difference between Normandy and southern Britain, as their is not a sharp climatic difference between Alsace-Lorraine and Baden-Wurtemberg. It is hard to believe that people from those neigboring regions are suddenly sharply intestinal differences due to genetic differences. Obviously something very important is forgoten: the cultural differences. We have to point that their is a cultural divide in Europe, especially concerning drinking habits. Globally we can notice three drinking Europes
1. Wine-culture Europe: in south-west: France, Italy, Spain and Portugal. If these countries are strongly oriented to wine it is not only a climatical question, because once again northern France has no real reason to be more wine-growing than the Germanic bordering regions. There are obvioulsy cultural reasons, as these wine-culture areas correspond also to the Latin European countries whose language are derived from Latin. Those areas were the center of Roman culture. It was the Romans that have brought wine from the mediterranean to northern Gaul when it was at that time a beer-drinking culture. wine culture then took roots in areas were it was not so natural to have it, while the neigboring areas of England or Germany, whose culture was moslty derived from Germanic/celtic cultures oriented on beer still as they were.
2. So the second Europe is the beer-culture Europe: British isles, Germany, central Europe. In some parts there exist a wine culture (south-western Germany), but it still is minority compared with beer-drinking culture. Beer drinking culture fit quite perfectly well with countries that are nowadays of Germanic language and culture.
3. The third Europe, is the vodka-culture in eastern Europe, and correspond quite well also with countries of Slavic languages such as Poland, Ukraine and Russia, etc.
There is nothing surprinsing that those three cultural groups correpond very well to the heart problems map, since it is known that daily consumption of red wine (as is done in France, Italy and Spain) has positive impact on it. Inversely heavy vodka drinking culture is obviously very bad for heart, while beer drinking is a bit less bad.

Very interesting association (as tight as the one as I have here). But I’m not sure that’s the explanatory variable. As far as I know, those in Anglo countries that try to adopt wine-drinking aren’t better off than others, and the overall level of alcohol consumption doesn’t vary all that much between the SW Europeans and others.
Diet may be key, but it’s probably so in terms of the evolutionary adaptations that that fostered in the people, and not so much what they eat/drink today. Intestinal length may be one of many such qualities.
“your explanaition might be interesting it doesn’t manage to explain the strong and sharp difference taht exist between the regions of the northern border of France and their neiboring German or English regions”
I think you’re right that it looks like three regions rather than two so maybe there are two reasons?
However taking what seems (from a layman’s point of view) like a good possibility i.e. the vasoconstriction point made above combined with the correlation with temperature – the original point made by the maps – then add in the effects of alcohol on vasoconstriction *and* on top of that the other obvious correlation with temperature and how adapted people are to alcohol and susceptible to alcoholism i.e. later agriculture because of the lower temperatures, especially regarding tolerance of spirits (and nb it’s not just vodka in eastern europe but whiskey in Scotland and Ireland) then
*if* the bulk of the difference between the “red” zone and the “yellow” zone actually occur in the coldest months then i think we may have a winner.
(the difference between the green zone and the yellow may be related to this somehow or have some other reason)
i love maps
The alcohol belt map is worth looking at.
Interesting find, thanks! It may be related, but is not quite as good of a fit. But, more data > less data.
Olive oil is the only source of fats in the diet that is known to be protective against heart disease. If you had a map which showed percentage of calories supplied by olive oil, I think it would match the crude death rate from cardio-vascular disease even more closely than temperature does.
The relation appears weak.
Is it really “protective”? Was that derived from suspect correlational studies?
I don’t think the relation is weak at all. I have no data of my own to offer, but as a long-time “health nut” who has read extensively on this subject, it is my impression that the correlation is robust. Olive oil is the chief component of the Mediterranean diet, and considering that it may be protective against heart disease explains the “French Paradox” as well as why Italian-Americans living in Chicago have low rates of heart disease. Low rates for heart disease among the French are paradoxical only if one thinks that butter is bad for your heart instead of considering the possibility that olive oil may be good for your heart. But the medical establishment has been wrong about the role of saturated fats in heart disease for nearly 60 years now. (Trans fats were the real culprit all along.) So I am not holding my breath until they decide to retract their erroneous opinions.
Olive oil consumption in France doesn’t appear to be all that high, though.
Oh wait. I didn’t realize that you were giving me link to the appropriate data. Have you tried running a regression using per capita consumption of olive oil as the predictor variable? Obviously, average winter temperature is not the real variable, but a proxy variable for something else which correlates with climate. My best guess is olive oil consumption. Others have suggested Vitamin D levels, binge drinking etc. If you have the data, regress all of these variables against the crude death rate from heart disease, and find out which of them explains the most variance. If you had a little finer resolution in the data, I m pretty sure you would find something interesting.
“Obviously, average winter temperature is not the real variable, but a proxy variable for something else which correlates with climate.”
What about the vasoconstriction point?
Anyway easy to show one way or the other – if the data is available. Does a significant amount of the difference between the red and yellow zone occur during the winter months?
Also worth considering is fish consumption (excellent source of Omega 3). Compare figures for eastern Europe (extremely low consumption) versus western Europe (3 – 4 times greater consumption): http://www.thefishsite.com/articles/contents/09-15-10art1.gif
http://link.springer.com/article/10.1007%2Fs11883-003-0086-y
Interesting. The thing is that it’s not clear that omega-3s are helpful, because a study of fish oil supplements found no benefit in those taking it. Perhaps very large doses are needed?
One more interesting article [“Wine, Beer, Alcohol and Polyphenols on Cardiovascular Disease and Cancer”]:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3407993/
“Would a burst of TMAO show up in people’s blood after they ate steak? And would the same thing happen to a vegan who had not eaten meat for at least a year and who consumed the same meal?
The answers were: yes, there was a TMAO burst in the five meat eaters; and no, the vegan did not have it. And TMAO levels turned out to predict heart attack risk in humans, the researchers found”
Any studies on the combination of TMAO and alcohol?
Sent this to a doctor in Finland, and she says:
In the 1960s Finnish men had the world’s highest death rate from heart disease. Heart disease was a problem all over Finland but the death rate was especially high in the province of North Karelia, an area in the eastern part of the country.
The people of North Karelia had a quite high level of fitness and smoking was not more prevalent than in other communities. However, the problem was in the diet. The region of North Karelia was dominantly farming and the consumption of high fat dairy products such as butter, cream, whole milk and cheese was widespread. The diet was also lacking in fruits and vegetables.
There have been major changes in dietary habits in North Karelia and Finland as a whole. The diet that used to be very high in saturated fat and salt now has one of the lowest fat contents in Europe and an average salt level.
Finland has reduced its incidence of heart attacks by 75% since the early 1970s. The mortality rates remain still quite high compared to some other countries but results have still been tremendous and this is clearly due to the reduction in risk factors. Of the single risk factors, reduction in serum cholesterol levels has had the greatest impact.
The full article here:
http://www.irishhealth.com/clin/ffl/finland.html
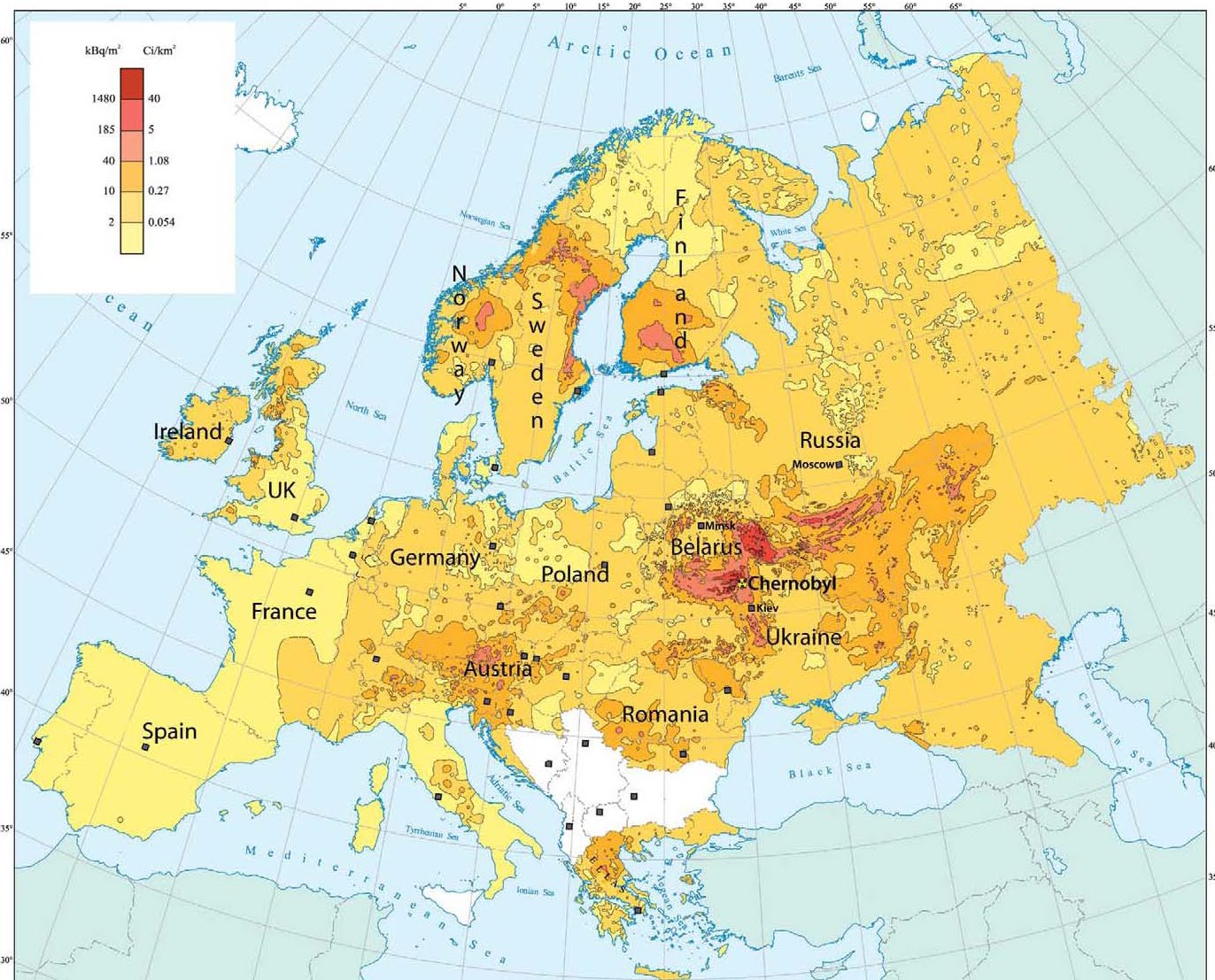
Try for this map, Chernobyl radiation levels in europe:
I asked this question on Razib Khan’s post about the fallibility of science but got no answer. Do you think the secondhand smoke studies are good science ? It seems some choices we make especially around health and diet have moral judgements attached to them . People who don’t smoke feel quite free to criticize those of us who do . It seems we’re one of the groups outside the pale of PC protection . Smokers can be ridiculed , discriminated against and attacked with public policy discriminating against them . The term “politics dressed up as science” comes to mind. I’ve found a number of places online that claim the numbers in second hand smoke studies are fudged and I suppose it seems plausible considering the relentless campaign against smoking. So I’m curious , what do you say ?
@donut:
If it’s an uncontrolled observational study, then it generally blows scientifically, so to speak.
Properly examining the effects of second hand smoke seems difficult, to me.
Thank you