
Features and Bugs
(This is also published at The Unz Review.)
A persistent misunderstanding both in the world of HBD and general medical and psychological science at large is the notion of what constitutes a “disorder.” When does a phenotype represent a physiological or behavioral malady? For behavioral issues, most people regard the Diagnostic and Statistical Manual of Mental Disorders (DSM) as the “final word” on this matter. While the DSM does make some attempt to assess actual impaired functioning, its assessments are tinged by cultural biases. A key component of DSM diagnostic criteria is social judgement of what is “proper” – what constitutes a correctly behaving person, according to the current cultural values?
Indeed, the DSM’s own Wikipedia page captures a many of the book’s problems:
Various authorities criticized the fifth edition both before and after it was formally published. Critics assert, for example, that many DSM-5 revisions or additions lack empirical support; inter-rater reliability is low for many disorders; several sections contain poorly written, confusing, or contradictory information; and the psychiatric drug industry unduly influenced the manual’s content. Various scientists have argued that the DSM-5 forces clinicians to make distinctions that are not supported by solid evidence, distinctions that have major treatment implications, including drug prescriptions and the availability of health insurance coverage.
But its more basic problems go deeper than that.
For starters, what do we mean by a “disorder?” The word implies that something is “out of order” – that is, something is not working as “intended.” Now when we’re talking about living things, that “intended” function is the function that survived the cruel process of elimination that is natural selection. Hence, any concept of a behavioral or physiological disorder must be informed by evolutionary theory. Medicine and psychiatry need to incorporate Darwinian processes.
As I begin, I want to be clear that it should be understood that all human behavioral traits are heritable, with “nurture” as its commonly thought of playing a minimal role to nonexistent role in each (see also Environmental Hereditarianism, The Son Becomes The Father, and More Behavioral Genetic Facts). The rest of this post proceeds assuming an understanding of this reality.
However, the people making these assessments, even the “experts,” tend to be evolutionarily illiterate; that is, they have a poor understanding of evolutionary theory. This failing isn’t just academic; in addition to hindering the understanding the nature and origin of these phenotypes, ignorance of Darwinism leads to to difficulty managing and treating them.
This means that there are a host of phenotypes classified as “disorders” that in fact aren’t, as well as a good many that are in fact Darwinian disorders which are not classified as such.
My Twitter followers know that I have been making noise about this problem for some time. And now, enter Durisko, Mulsant, McKenzie, and Andrews, 2016, with their paper “Using Evolutionary Theory to Guide Mental Health Research,” published in The Canadian Journal of Psychiatry.
The authors (who I suspect have read my writing) sum up the problem excellently in their abstract:
Evolutionary approaches to medicine can shed light on the origins and etiology of disease. Such an approach may be especially useful in psychiatry, which frequently addresses conditions with heterogeneous presentation and unknown causes. We review several previous applications of evolutionary theory that highlight the ways in which psychiatric conditions may persist despite and because of natural selection. One lesson from the evolutionary approach is that some conditions currently classified as disorders (because they cause distress and impairment) may actually be caused by functioning adaptations operating “normally” (as designed by natural selection). Such conditions suggest an alternative illness model that may generate alternative intervention strategies. Thus, the evolutionary approach suggests that psychiatry should sometimes think differently about distress and impairment. The complexity of the human brain, including normal functioning and potential for dysfunctions, has developed over evolutionary time and has been shaped by natural selection. Understanding the evolutionary origins of psychiatric conditions is therefore a crucial component to a complete understanding of etiology.
Durisko et al produce a neat chart that analyzes examples:

The sad fact of the matter is that there are some disorders the medical and psychiatric communities are correct in calling disorders but these communities are ignorant about why they are correct. These lead me to the first major cause of mental disorders.
A major challenge any functioning organism faces is genetic load. This is the burden of deleterious mutations that we all carry. For a discussion of this, see Greg Cochran over at West Hunter:
Typos
Get Smart
More thoughts on genetic load
The genetics of stupidity
The Golden Age
In short, new mutations always arise. The majority of these mutations are neutral or harmful to fitness. Deleterious alleles are selected out at a rate proportional to their fitness impact; the bigger the fitness hit, the faster they are selected out. This means that alleles with mild fitness impacts can persist for many generations. Certain individuals can have more than their fair share of the these deleterious alleles. In some cases, this leads to mental illness – when there are just one too many things “broken” in the brain. While the individual alleles that are causal to these illnesses are all rare and are all being selected out, new mutations continue to arise, hence, the illness persists in the population – each instance being genetically distinct from all the others.
Mathew Keller and Geoffery Miller detailed how this applies to mental illness in their 2006 paper. Genetic load largely* explains mental illnesses such as autism, schizophrenia, and bipolar disorder.
Since men generate sperm throughout their lives, older fathers pass on more mutations to their children. Hence, paternal age can be used to gauge the effect of de novo mutations on a phenotype, which is a clue to how much genetic load is involved. Autism, schizophrenia, and bipolar disorder all show paternal age effects – that is, older fathers are more likely to have children with these afflictions (D’Onofrio et al 2014). These conditions are true disorders in the Darwinian sense, although research continues into the genetic architecture of these phenotypes. They are bugs, not features.
So the psychiatrists got these right. But, as we see above, there a host of “disorders” that they got wrong.
The biggest category here are the personality disorders, of which, psychopathy (or “antisocial personality disorder”) being the most prominent. (A review of the heritability of these personality disorders can be found here: Reichborn-Kjennerud 2010.) The rationale for categorizing these phenotypes as disorders in the DSM is as described quite well by Durisko et al (emphasis mine):
The DSM-5 defines mental disorder as “dysfunction in the psychological, biological, or developmental processes underlying mental functioning.” … (p20) and operationalizes this dysfunction with proxies such as the inability to work, maintain interpersonal relations, and take care of one’s self. Several authors have pointed out the difficulty this approach can have in distinguishing between normal and abnormal behaviour …
Distress, impairment, and inability to function in everyday life [that is, in modern society] are not necessarily indicative of biological malfunction … The normal functioning of the body’s evolved systems can at times be unpleasant and cause suffering.
Durisko et al go on mention childbirth as an example of a biological function though it causes pain and suffering even when it operates as it should, and that’s a good example. I will add that social undesirability is of course another factor that colors the DSM classification, as psychopathy illustrates perfectly.
Many of these “personality disorders” embody phenotypes that are continuously distributed in the population. My earlier post Predictions on the Worldwide Distribution of Personality illustrates this to an extent. For example, both anxious and psychopathic tendencies are not distinct categories but rather are continuously distributed in the population. Anxiety appears to relate to the HEXACO Emotionality and perhaps low eXtraversion. And the psychopathic traits are well represented by the Dark Tetrad, which is its own dimension (Honesty-humility) in the HEXACO. What we call “psychopaths” are just individuals who score above an arbitrary cut off on the Dark Tetrad dimension. I have argued that the prevalence of such traits is related to clannishness. What the authors of the DSM have done with most personality disorders is “pathologize” points of normal personality variation that don’t conform to the (very WEIRDO) ideal. These traits are adaptations nonetheless. Psychopathy is a feature, not a bug.
In the chart above by Durisko et al, they talk of “alternating selection” as maintaining many of these traits. Psychopathy (at least in WEIRDO environments – see the list in the beginning of the post Clannishness – the Series: Zigzag Lightning in the Brain) is commonly thought to be maintained by frequency dependent selection; that is, psychopathy is adaptive at low frequency but becomes maladaptive when it becomes too common.
I suspect that the general idea is correct. However, let me interject here that most discussion of the evolution of human traits ignores recent selection. There is group-level variation resulting from regional differences in selective pressures. To quote Greg Cochran, “every society selects for something“, and what that something is varies by time and place.
Hence, a lot of these ideas on the evolution of human behavioral traits (including the personality “disorders”) suffer from WEIRDO bias. For example, the”optimum frequency” of psychopathy varies from population to population – being much higher in clannish societies.
Indeed, Penke, Denissen, and Miller (2007) claim this is true for all personality traits. That is, variation is human personality is maintained by frequency-dependent selection, with most personality traits being most adaptive when they are found at intermediate frequencies. Of course, as per the above the optimum frequency for each personality trait will be different in different societies. These explain the group-level differences we see in most behavioral traits.
But aren’t there times when the extremes of something which is continuous distributed is bad – too much of a good thing, as it were? Sure. One example may be hoarding. As Cochran explains:
It could be that people, at least some people, just feel like saving, and would do so even if it were economically irrational.
…
It looks as if saving has had a bigger payoff in recent millennia than it typically did in the distant past. I’m not say that as an iron law, more as a tendency. There may have been ways of saving food for hard times (winter, mainly) quite a while ago, at least in cold climates… at least you’d think so.
…
Farming must have favored low time preference.
…
Grain crops can be stored, and seed must be saved for the next growing season.
…
where saving had higher payoffs, individuals that had a greater innate propensity to save ought to have had higher fitness. Having lower time preference, acting more like homo economicus , may have been favored, but surely a simple hoarding tendency, more like a squirrel burying nuts for the winter, would have been favored as well. Maybe there was selection for being more of a squirrel…Of course there is a distribution of such traits, ranging from a little to a lot. In a population with a greater mean amount of tendency-to-save, some would do so to a ridiculous extent. Hoarders. They may not be equally common in every population.
Anxiety “disorders” may be similar to hoarding in this way. People with extreme levels may just be the unfortunate beneficiaries of genes that were adaptive in their ancestral environments – albeit at more moderate levels.
Speaking of ancestral environments – sometimes a “disorder” arises because of a mismatch between the modern environment and the ancestral environment. An example would be altitude “sickness.” Individuals whose ancestors lived near sea level can have trouble in the lower atmospheric environment found at high altitude, and they exhibit all manner of maladies when at heights. Here it’s clear that there is no actual disease present; rather the sufferer is outside the environment in which they evolved.
Substance addictions are shining examples of such phenotypes. Typically, the addictive agent was not present in the sufferer’s ancestral environment. Hence, when exposed to a world that has tobacco, cocaine, or alcohol, for example, they can become addicted.
Addicts remain in some societies that have had the offending substance for some time because selection against such afflictions is ongoing. We can see this in action when we look at Europe (from here):
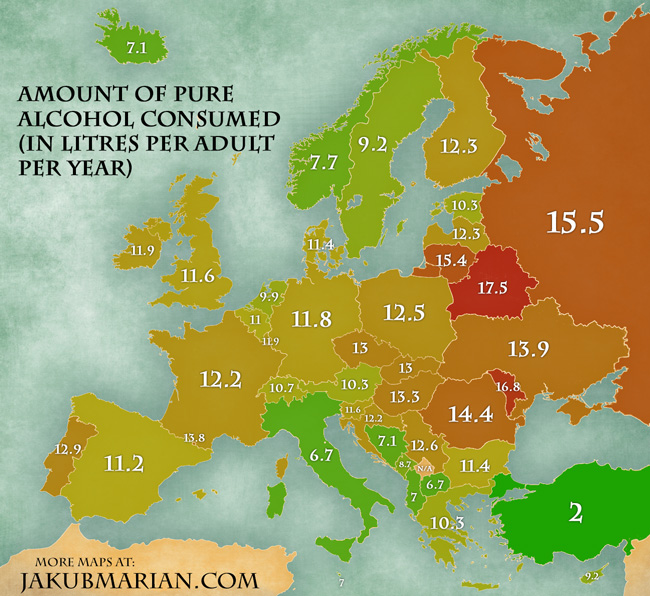
Alcohol consumption in Europe inversely correlates with the length of time each society has practiced agriculture (from here).

See also Firewater | West Hunter.
Type II diabetes and perhaps irritable bowel syndrome may also be examples of these types of phenotypes. Afflictions that stem from environmental mismatch aren’t “disorders” in the Darwinian sense. Rather, there are a turnover in direction of natural selection.
This also, by the way, highlights a key fact about the aforementioned genetic load. There is a key difference between afflictions stemming from environmental mismatch and disorders stemming from genetic load (such as autism, schizophrenia, or bipolar disorder). Where as the genes that cause substance abuse or altitude sickness are clearly adaptive in some environments (ancestral ones) and were selected for by evolution, the genes that lead to autism, bipolar disorder, or schizophrenia are maladaptive in any environment.* Disorders caused by genetic load are true Darwinian diseases.
The reality of environmental mismatch puts the kibosh on a popular concept in the alt-right sphere, referring primarily to Northwestern Europeans: that is, “pathological altruism.” Specifically, some in this space view the universalist acts of Northwestern Europeans – such as inviting refugees and other immigrants from poor and/or war-torn Muslim countries (despite the higher crime rate and lower socioeconomic performance of these immigrants) – to live in Northwestern European countries as a type of pathology – i.e, a disorder. As Jared Taylor put it (emphasis mine):
We will turn our backs on our own group in the hope that members of other groups will do the same—despite clear evidence that other groups have no such intention.
A somewhat less deceived writer advises that if groups want to act altruistically towards other groups they should at least look for groups that follow the same rules. But this is as far as the book goes. Group pathology leads only to mistreatment of out-groups. Apparently none of the authors can conceive of pathology in which the in-group mistreats itself for the benefit of strangers.
Yet, of course, it is not a disorder. “Pathological altruism,” at least when used to refer to this aspect of Northwestern European behavior, is a silly term.
As I detailed in my post The Rise of Universalism, the universalist behavior of Northwestern Europeans is a natural consequence of their special flavor of reciprocal altruism, which is not strictly kin-centric and views all people (indeed, often non-humans as well) as potential recipients for sympathy. In that post, I explain how modern technology led to an inevitable increase in universalism among Northwestern Europeans – that runaway universalism was inevitable. Clearly an inherited phenotype can’t be a pathology when it is possessed by sizable fractions of the populations under consideration. Rather universalist sentiment is a feature, not a bug (or more accurately, it is the result of a feature). It’s not even clear that such traits even have a direct negative fitness impact, as it’s not yet been established that such individuals aren’t the most fertile in these countries (though it appears to be presently deleterious in the United States).
Finally, as noted, just as there are phenotypes that are (for cultural reasons) classified as disorders that are in fact not, there are afflictions that are not classified as disorders that in fact are. Most poignant of these is obligate male homosexuality. The DSM long since removed it from its list of disorders. Yet there is no environment where lack of interest in the opposite sex is adaptive. It is literally a Darwinian disease. Yet, homosexuals make up 2-5% of the male population – a far greater fraction than the sufferers of disorders like schizophrenia. Genetic load is unable to explain the existence of such a common fitness-reducing disorder. The only workable explanation for such a common fitness-reducing disorder is a pathogen.
As detailed by Greg Cochran (as collected in Greg Cochran’s “Gay Germ” Hypothesis – An Exercise in the Power of Germs), the proximate cause of homosexuality is likely damage resulting from an infectious agent. Numerous facts support this, including the very low heritability (< 22%, in stark contrast to most everything else). Indeed, pathogens are the other important source of human maladies, both physical and behavioral. Many diseases that don’t fall under the above category may be found to have pathogenic involvement*.
The primacy of sex drive and sexual reproduction to fitness (without it, little else really matters, evolutionarily) means that evolutionary theory can be used to evaluate other claimed disorders like – asexuality. True asexuality – a complete lack of interest in sex – would be as much a Darwinian disease as would homosexuality, at least for men. This would lead us to expect it to be very rare. And indeed despite earlier claims to the contrary, such appears to be the case (Cranney 2015).
The importance of sex drive is another reason to doubt another claimed disorder (that fortunately didn’t make the DSM V): sex addiction (aka “hypersexuality”). Sex drive is continuously distributed across the human population. This lends itself to the use of arbitrary cutoffs when declaring “pathological” states. Indeed, one Croatian study found that self-professed hypersexual men weren’t all that more sexual than men who simply claimed to be highly sexual – they just feel more ashamed about it. Now, as mentioned above, although continuously distributed traits could lead to “pathological” extreme cases (e.g. hoarding), there doesn’t seem to be much support for this notion in the case of sex addiction.
There will likely always be a level of subjectivity in what human phenotypes we label “disorders.” But at least by proceeding from a Darwinian model, we have a framework with which we can have a reasonable understanding of human disorder, and not continue to make things up to extent we presently do.
 *I mentioned the role of pathogens in the existence of persistent human disorders. Greg Cochran and Paul Ewald make the case in their 2000 paper that genes for certain human maladies may stick around because they confer defense against pathogens. Hay fever may be a poignant example of this (Tyagi et al 2015). This may also be true for some genes that cause certain mental disorders.
*I mentioned the role of pathogens in the existence of persistent human disorders. Greg Cochran and Paul Ewald make the case in their 2000 paper that genes for certain human maladies may stick around because they confer defense against pathogens. Hay fever may be a poignant example of this (Tyagi et al 2015). This may also be true for some genes that cause certain mental disorders.







I am not convinced by the argument against “pathologists altruism”. First, there is certainly a point beyond which altruistic behaviour is harmful to the individual practising, either from the personal point of view, or from the point of view of genetic fitness. Second, it is never adaptive to lose the ability to discern, at least roughly, where that threshold lies. Third, even if a practice seems adaptive in the short term, because it’s propagation coincides with population growth and/or an increase in material well-being, that is no proof that it is truly adaptive. The apparent flourishing might only be a prelude to catastrophe, as when shoots that arise too early are killed off by frost.
“Pathological altruism”, I mean, of course.
That’s true for most personality traits.
You do know what “fitness” means, right? It means maximizing the number of descendants you have.
Yes, fitness = maximizing your descendants. The thing is, something can seem to increase your fitness in the short run, while in fact having a sting in the tail that decreases your fitness in the long run. To illustrate the point, suppose a woman had a mutation that caused her to have litters instead of one baby at a time. This could dramatically increase her number of offspring. But suppose the same mutation caused the babies to be sterile. In the long run, the woman will have no descendants. What seemed to increase fitness would in fact have decreased fitness.
Then such a mutation is actually decreasing her fitness, is it not? Don’t forget to iterate.
Yes, it’s decreasing her fitness, that’s the point. I was arguing that a trait can seem to be increasing fitness when its not, the illusion being the product of, e.g., observing its effects over a too-short duration.
I think your idea of a disorder commits the naturalisitc fallacy. The very notion of a disorder is normative. It’s a mistake to think that this normative evaluation can be derived from Darwinian facts. There are fitness-reducing traits, but whether any of these deserve to be called “disorders” cannot be settled in the lab. Atheism, high intelligence and advanced education in females are fitness-reducing traits – or at least correlates of such traits – but they are obviously not disorders. “Fitness-reducing trait” is not such a terrible mouthfull, and a very useful concept in science. By trying to use it as a basis for some naturalistic analysis of “disorder”, you needlessly sew confusion into both the scientific debate and the normative debate. Let’s not.
I know my posts are long, but it’s really annoying when critical commenters don’t bother to to read them.
Disorders are phenotypes that are maladaptive in any environment. Things that were adaptive in the past but no longer are aren’t, as I explained.
Yes I’m arguing for a semantic change, but one based on a solid natural foundation. It’s a good idea to set your clocks by the Earth, Moon, and Sun (the day, month, and year, respectively), at least to start.
The whole point of “disorder” is that it deviates from the norm, one of the 4 “d’s” of abnormality in abnormal psychology. There is deviance, distress, dysfunction, and danger. For something to be a disorder, it must deviate from the norm, cause distress to the individual, as well as dysfunction and finally be dangerous to the individual or the population at large.
Though, some researchers dispute that abnormalities exist. They claim that “deviance in one culture is normal in another”. For instance, my professor said, when asked about deviant behavior, said that someone not taking a shower is a sign of dysfunction. She then said that in some cultures that going for a long period of time without showering is normal in their culture, but it’s deviant in ours. I immediately said “I don’t care what culture that is. If you don’t shower for a week, you’re dirty.”
It’s pretty subjective, like most of psychology, except for IQ tests of course, one of the only things in psychology that can be replicated again and again, in comparison to the other 80 percent of things that cannot be replicated.
That’s why a Darwinian approach is better. And I think “disorder” as in “something is out-of-order”, as in “broken” makes more sense.
Agreed fully. Whatever behaviors we have culturally (which we know is just a product of genetics), there has to be some sort of “normal” for every human population.
For instance, if there was a population of humans somewhere in the world where, lets say, schizophrenia is the norm, would that be normal to them and abnormal to us if they could function and still increase their fitness by spreading their genes to the next generation?
I think abnormal psychology is pretty useless. Don’t even get me started on Freud.
I must say, JayMan, this is one of my favorite articles from you. I’m going to email this to my abnormal psychology professor after I’m done with this semester. She gushes over the DSM V. As well as gushes over Freud (ugh). I’d love to see her reaction.
So in a Darwinian perspective, what would you constitute as a disorder?
In a nutshell, your position is that mental illness is simply behavior that is outside what amount to subjectively-set boundaries, and that the spectrum of such behavioral traits may often have plausible explanations in the evolutionary sense.
Seems right to me. Since mental illness is not specifically like a brain tumor and behavior is certainly coded by the genetic software and hardware of the brain, I find the entire medical model inappropriate and the “medical treatments” for most disorders appear very troubling to me (most notably anti-psychotic medications, whose effects are apparently bad and side-effects possibly worse than the original disorder.
Many people with serious behavioral aberrations still make it through their reproductive years, which suggests that the pressure to remove even significant perturbations from the gene poll is low. No wonder “all the bitches, they be crazy.”
Yes, but not because they were specifically selected for. A good many of them are mistakes – results of mutations or other disturbances as described.
True but there is much more to evolutionary fitness for humans than living long enough to breed. Sufferers of mental illnesses (like autism and schizophrenia) do indeed have substantially reduced evolutionary fitness.
Autism is also a spectrum. Seems to me that as the industrial revolution happened, we needed more men to design ships and steam engines and radios, that therefore having a moderate degree of autism becomes a slight advantage, causing one to spend less brain power computing social hierarchies and instead focusing on the draft table and the laboratory. Similarly, we can see a correlation of schizophrenia and creativity. Could it be that genes for these things are advantageous in small amounts, reduced fitness in large amounts?
No, it’s not a spectrum. More on that later.
Autism is also correlated with high IQ, as well as schizophrenia doing the same. So there’s basically, as they’ve been saying for years, “a fine line between psychopath and genius”.
Not really.
Actually, that correlation is decidedly negative, even between MZ twins.
Really? I’ve read a few studies that said that it is. Got some links for me? Same with schizophrenia. I’ve read a few things about that in the past few weels.
Much appreciated.
For schiz.
I’m curious to hear more on the homosexuality bit, because there are some studies that try to find some form of a gay gene – Xq28 – though replications haven’t been in order, though a few times every year a page boasts that they have found it. There was also a study by an Italian researcher on how homophobia was a mental illness, though the researcher couldn’t be bothered to explain how a maladaptive behaviour being shunned is somehow bad – of course, as it was a political based paper, it got published. As you say, any discussion on homosexuality is bound to be worthless. If it isn’t positive, it won’t get published. Same with any studies on transgenderism.